COMMUNITY MEDICINE (2 months)
I've started year 4 with Community Medicine posting. Who said this posting is the most relaxed one? They all are totally wrong (haha jkjk). Okay okay, I can say this posting is the only time I can relax from hearing & remembering those medical terms. But this posting has its own challenges despite its so-called "Honeymoon posting".
 |
| During our visit to Hospital Pekan |
Dr Pius thought us very well in this posting. I guess this is his last time teaching students because he already retired before he teaches another group. In this posting, we were busy with research & visits. We're doing research on Obsessive-Compulsive Disorder(OCD) on attendees in several Klinik Kesihatan in Kuantan.

We assessed their knowledge about OCD. Sometimes they told us about their real OCD experience, either themselves or dealing with family members with OCD. Some people didn't know it was a disorder. Their family members often hoard certain things, even one of their family members washed their mobile phones because of their paranoid toward germs until their phones can not be used anymore(unbelievable tho !), some people renew their prayers (angkat takbir berkali-kali), renew their ablution or in Malay term --> was-was . In Islam, Holy Quran has one surah called surah An-Naas, which we're advised to read this surah whenever we feel doubt about the things we do every day:

From the mischief of the Whisperer (of Evil), who withdraws (after his whisper),-
(An-Naas 114:4)
For me, it was a challenging yet meaningful experience cuz we learned a lot while doing this research. We "play" with data and laptop all the time (I almost wear specs because I spent most of the time on laptop and analyzing data 😭). We used IBM SPSS Statistics apps for our data manipulation. It was not easy in the first place cuz we thought we can use an online form to do this research but our lecturer encourages us to do field work-study instead of online because Dr. Pius told us that we need to learn new experiences while doing our research. And what he said is totally correct because we can enhance our communication skills while collecting samples for our study this time. We need to collect about 200+ samples for our research in 3 Klinik Kesihatan in Kuantan. I worked with 5 other members of our group so I need to collect 30+ samples from attendees in KK myself.
 |
| The first stage of research: retrieving Literature Review really gave us headache😭 |
 |
| Before submitting our Research to our lecturer. Such a satisfying moment I guess. I'm grateful to have such an amazing team on this research! Bravo guys |
 |
| Brainstorming our ideas : all about OCD. It's totally worth it ! |
As a student who studied in a private institution, I admit that we have to do everything on our own. in other words, we have to be independent students. We were assigned to contact each department by using official letters by ourselves. From this experience, we learnt how to make official letters to the government & private sectors including JKNP, PKD, PAIP, Jabatan Alam Sekitar, factories and etc.
We were exposed to hierarchy of Ministry of Health through Kuantan District Health Office ( Pejabat Kesihatan Daerah Kuantan) & Pahang State Health Department ( Jabatan Kesihatan Hegeri Pahang ). PAIP, Pusat Pelupusan Sampah Alam Flora Jabor. PKD is more concerned with community health in Pahang such as dengue, malaria, leptospirosis, or any outbreaks in Pahang.
 |
| Hospital tour in Hospital Pekan |
 |
| Our visit in Klinik Kesihatan Beserah (the largest KK in Kuantan, I think it was KK Tahap/jenis 2) |
 |
| Our visit in JKNP |
We also visited an electronics factory to observe how a company took care of their factory worker & put their worker's health on the first line. They bought PPE (different boots, ergonomic chairs, ear muffs, eye protectors). We observed how their work can cause long-term health issues such as carpal tunnel syndrome, hearing loss, asbestosis and etc. if they don't take precautions, PPE will minimize the long-term health side effects from their workplace.
 |
| exhibition section |
 |
exhibition section
in the factory(ruang pameran) |
 |
| our fav part after the factory tour was --> EAT 😋 |
 |
| TT electronics factory |
We have also done visiting Air Pollution Index Centre in Indera Mahkota, and we observed how they collect the air index data from the post located in one school in Kuantan. We watch how they display the reading in the information centre.
After that, we visited the water treatment plant and observed how they process the raw water until it becomes crystal clear clean water to be used by the household & community.
 |
| Our visit to pusat rawatan air in PAIP |
 |
| The instructor explained how the water treatment was done in PAIP |
 |
| In PAIP |
We went to a dumping site managed by one of a company in Kuantan under Jabatan Alam Sekitar, and learned how they process solid waste. We were shocked by how much the government had to spend to process solid waste. we were reminded of how important the 3R(reduce reuse recycle) is not just to minimize the cost taken to process the solid waste, but also to our nature too. we've learned what if all these companies didn't exist, how the community will live without them and we can see how important their role is in the community. Near the dumping site, there is a water sewage treatment plant. The sewage water released from the dumping site is collected, processed, and treated before being released to the lake.
 |
| Landfill in Jabor. We get ourselves our own boot to come here. We also need to wear a face mask, trust me, even 2 ply of the mask will not stop the smell, so stop wasting them 😆 |
 |
| In the water treatment plant |
 |
| The sewage from the landfill was collected and purified before they release it into the lake |
 |
| A pack of dogs and a flock of birds were seen in the landfill(hati2 k !) |
Klinik Desa
I don't find any picture for this visit lol. So we just learnt that Klinik Desa only cover Antenatal simple check-up and usually Jururawat Masyarakat(JM) & Medical Assistant will standby here. There is no doctor in Klinik Desa , so all the detailed check-ups must be done in Klinik Kesihatan.
FAMILY MEDICINE POSTING (4 weeks)
One of the best postings in year 4. Our legendary Dr. Khairi taught us during this posting.
In 4 weeks, we were in KK Kurnia most of the time. We were divided into 4 more groups: mother & child health(MCH), clinical lab, outpatient department, procedure room. We all rotated within 4 weeks to fill in all the cases seen & procedures done in our logbook.
 |
| While waiting for patients in the outpatient area |
At 11am, Dr will ask us to present cases every day in the seminar room in KK. In the evening, we will come over to our lecturer's house to do seminar there
In clinical lab, we were given the opportunity to help the medical lab technologist (MLT) to do urinalysis(UFEME), full blood count(FBC), rapid blood sugar(RBS), erythrocyte sedimentation rate(ESR), bilirubin level for NNJ, Ziehl-Neelsen staining for TB.
 |
| I was doing a urine dipstick test |
 |
| Aminah - while waiting for the result for UFEME |
 |
| MLT was doing Ziehl-Neelsen stain for TB |
MLT was doing Ziehl-Neelsen stain for TB
 |
| 10 gram monofilament. Used in physical examination in DM patients for neuropathy(get used to it cuz it was Dr. Khairi's fav question for exam heh) |
 |
| Antara lecturer yg tak pernah berkira dgn kitorg. Our father here. Belanja makan, shell out, durian, even arrange our trip to Tasik Kenyir. He was the one yg push supaya our college make a proper Oath Taking Ceremony every year. May Allah bless him til the end :) |
 |
| One with our MLT |
In MCH, we observed antenatal ultrasound, vaccine administration for babies, family planning clinic, heel prick test for neonatal jaundice (NNJ), MOGTT, antenatal ultrasound.
We clerked many patients with different backgrounds/social/medical histories. But one story of the patient still lingered on my mind until now. I clerked a patient who came for family planning without her husband knowing. Initially, she came for depo-provera contraception injection, but the doctor couldn't give the injection because of the side effect of her previous injection which already caused her to have a dangerously spiking blood pressure. I asked her why both of them didn't use a barrier method or pills? and the next word she said breaks my heart😭 : HER HUSBAND DIDN'T ALLOWED IT ! What the.... 😡 the fact that she came to the clinic without her husband knowing about that already made me suspicious. She secretly takes oral COCP, but once her husband finds out, he throws away the pills and warns her to never take them ever again. She is already tired of taking care of their >5 children, please have a conscience. From all the things that I learnt in medicine about contraception, most of it is on women, which most of them cause various unpleasant side effects. I'm not being a feminist here & I know that not all guys are the same, but this story totally breaks my heart. Dear husband, before marrying your wife, please find out what is the purpose of marrying your wife. That's all I can say.
 |
| I help the nurse to prepare drinks for the modified oral glucose tolerance test (MOGTT) P.S. : this was also fav question on how to diagnose GDM in O&G |
 |
| the drinks come from a sachet form of 75gram of glucose |
In the Procedure room, we observed & learnt a lot of procedures from very helpful medical assistants such as blood taking, dressing, preparing a nebuliser for asthmatic patients, etc.
This is my first time encountering a patient with gonorrhoea(one of the Sexual Transmitted Diseases). For clerking STD patients, we must pay a lot of attention to their social history and background, their behaviour, etc. Otherwise, we will miss the diagnosis and the appropriate treatment couldn't be given due to our lack of skills.
Methadone clinic - we were exposed to how Methadone clinic works in Klinik Kesihatan. It was located outside or further apart from the other area of the clinic to give privacy to the drug addicts due to the social stigma. Methadone is an initiative by the government to reduce HIV transmission or other blood-borne viruses that transmit by sharing needles. So, Methadone will be given to the drug addicts according to dose, even though it will still cause addiction, but it significantly reduces the risk of HIV transmission as I mentioned above. If the drug addict was caught by the health workers with positive urine with other types of drugs, the Methadone will not be given & their case will be handled by the police. We also taste a drop of it, (because the MA said we shouldn't be conned easily by the drug addicts, so we should taste it lol haha) so the taste is slightly bittersweet. The reason they put sugar in the Methadone is to prevent the drug addicts from self-injecting Methadone into their bloodstream because the sugar will crystallize and will clog the syringe. And if they were caught re-selling the Methadone, the health workers will not hesitate to give them to the police.
Outpatient department - we have to clerk cases & present the cases to the MO in order to get the stamp chop and signature for our logbook. I took an opportunity to do a medical check-up here with MO here after we did our own FBC.
This is one of my favourite postings 💚 & I even consider becoming an MO in KK settings or continuing my study in FMS hshshs but we never know how our future works right. Just pray & hope for the best in the future.
ORTHOPAEDIC POSTING (6 weeks)
Abbreviation used in this posting : fracture(#), open reduction internal fixation (ORIF), posterior/anterior collateral ligament(ACL/PCL), medial/lateral collateral ligament(MCL/LCL), neck of femur(NOF), below/above knee amputation(BKA/AKA), total hip/knee replacement (THR/TKR), rheumatoid arthritis(RA), osteoarthritis(OA), osteomyelitis(OM), diabetic foot ulcer(DFU), motor vehicle accident(MVA), avascular necrosis(AVN), distal radioulnar joint(DRUJ), compartment syndrome(CS), range of movement(ROM), Disease-modifying antirheumatic drugs (DMARDs),Volkmann ischemic contracture(VIC), cancer(Ca), giant cell tumour(GCT), multiple myeloma(MM).
This posting was quite busy because we had to enter ward, clinic, OT all over again, just like Surgical & O&G postings. We also need to attach in the rehabilitation centre & prosthetic clinic this time.
Most of the patients in this ward were male. Because many of them are involved in road traffic accidents. During 1st time I enter the ward, I was quite fascinated (plus scared fr!) while witnessing all skin/skeletal traction, external fixator, Ilizarov fixator, Halo vest, etc. During this posting, I admit I ride my motorbike slower than usual & be a responsible rider cuz I was afraid of the consequences lol.
 |
| Ilizarov fixator |
 |
| Halo vest |
 |
| skin and skeletal traction |
 |
| external fixator |
We follow ward rounds and bedside teachings with our specialists after their office hours, sometimes, our ward rounds finished at 11pm ! phewww.
In the clinic, we attached with MA in the procedure room where we observed on how the medical assistant do & removal of a cast.
In OT, we need to wear a heavy plumbum gown throughout the surgery, because the portable x-ray was used during the surgery. After a few hours, you might get back pain okkk I'm not joking.
 |
| Plumbum gown |
In rehab, we observed how the patients did their rehab and how they made prosthetic legs(not exactly, it just how they wear it, is it fit or not sth like that)
 |
| Procedure before prosthetic leg was made, The prosthetist will make a mould, and will send the prototype to the factory |
 |
| Rehab for pediatric cases such as muscular dystrophy, cerebral palsy, developmental delay, or hip dysplasia |
 |
| Rehabilitation department |
 |
| Rehabilitation department |
 |
| Rehabilitation department |
 |
| Amazing rehab pool isn't it? Rehabilitation department |
 |
| Procedure room in Ortho clinic |
There are so many scores & classifications in Ortho that you need to remember. So, you better make the notes earlier.
During end of posting exam, I messed up during shortcase. I got a diabetic foot ulcer(DFU) case which I didn't practice that much. My tips are, don't panic, don't forget your gloves while doing the palpation, don't stutter. I got a spine case: vertebral fracture for longcase. I was quite panicked lol cuz we didn't cover spine cases that much due to the tight schedule during our posting. Alhamdulillah, I passed it with flying colours because the examiner was so kind and just asked me to show the cutaneous innervation of the lower limb from the spinal cord after presenting my patient's history and doing PE.
 |
| With our lecturer in front of Ortho ward after we finished our exam. Finally the end of a longgg posting in year 4 |
 |
| Suture session |
 |
| Suture session |
 |
| POP application session |
 |
| POP practice session |
 |
| POP practice session |
FORENSIC POSTING (3 weeks)
Forensic was one of my favourite posting cuz I can rest from those difficult medical terms and we could learn a whole new experience here. Forensic is always a taboo posting from what I've heard from the seniors. Because it involved a deceased person instead of a living person in other ward/postings. The forensic department in HTAA is small and the mortuary room is very limited space. We need to wear an apron, mask and shoe cover before entering the postmortem room because the blood might be spilt from the bodies.
 |
| Goodbye to one of the best postings and lecturers from the Forensic Dept. |
We observed 4 postmortems so far within 3 weeks of our posting here :
CASE 1 : A young military male (sudden death) --> Acute Myocardial Infarction
CASE 2 & 3 : A young mother and her daughter died from a motor vehicle collision
CASE 4 : A middle-aged male died from a high-speed motorcycle collision
I still can remember the surroundings vividly while I'm writing this. I still can remember the griefs from family members in the mortuary. We as students need to respect what the family members felt by keeping ourselves silent when passing through the family members in the mortuary.
Usually, we need to standby during the weekend and night cuz usually there is an accident during these times. In the 2nd & 3rd case, it was in the middle of the weekend night when our specialist asks us to come to the hospital to observe 3 postmortems.
We were once invited by our HOD to observe a postmortem of high profile case in Genting Highland which was a murder case. But unfortunately, we couldn't make it to the place so we just heard the postmortem from her. Whenever there is high profile case, only our specialists knew the details about the case where the media didn't expose it cuz sometimes it involves politicians or high ranking groups in the country.
Let me tell you guys how is it like to be in the postmortem room. There is 2 table for the bodies, there is one table that is filled with this equipment:
 |
| there is a long knife, rib breaker(uhh, I don't remember the real name duh), large needle, stitch(to stitch back the body) |
Before autopsy, the bodies were photographed by the police for their records, after that it was handled by the doctors. Firstly, the doctor observes any bruises/cuts/lacerations from the skin. And then, Y-incision was done to take out the internal organs. A machine that we called a "skull cutter" is used to take out the brain from the skull. After the doctors take out all the organs, we weigh each of them to rule out any abnormalities such as heavier lungs may indicate pulmonary edema etc. After that, the doctors slice each of them to observe any blood clot or ischemia (mostly in the brain/heart/lungs). All the specimens from each organ were sent to the pathology department for further investigation. The doctor also counts how many ribs/bones were broken in MVC cases. After all the procedures, the organs were put back into the bodies and were stitched with a large needle and some kind of thick thread.
The doctor draws all the findings in 1 paper for medical reports while doing the postmortem.
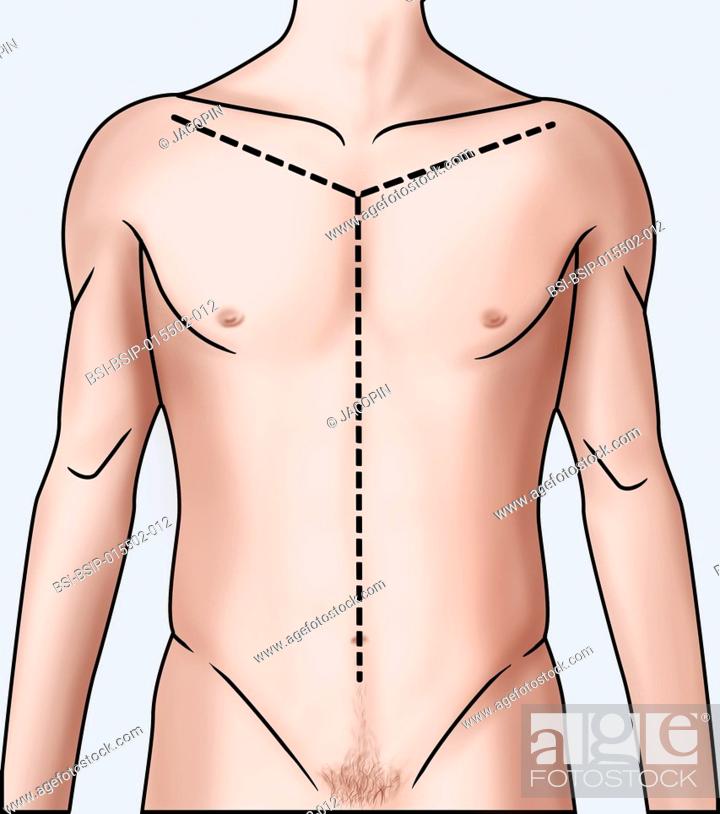 |
| Y-incision |
Maybe many of you guys wonder, how is it smell like. For the fresh bodies, it smells like raw chicken. But, if the body was found out after 3 days, it may smell like a corpse and the smell will attach to your cloth eternally (jkjk). For the previous group, our friends don't dare to eat any chicken after the postmortem, but for us, we don't care cuz we are hungry to death after each postmortem, cuz it takes long hours 😂 so we just eat what we want afterwards lol.
 |
| full attire when entering the postmortem room |
 |
| after a long-standing hour haha collapsed |
 |
| One of my fav topics: firearm injury by shotgun |
We've learnt so many interesting topics, even though all of it was theories, but it was enough for me cuz it was so interesting from the beginning. Some of the topics were: blunt & sharp weapon injuries, firearm & explosion deaths, road traffic collision injuries, writing medico-legal reports, court procedures for doctors, death from poisoning and drug abuse, asphyxial death notes such as in suicide/drowning, etc.
At the end of 3 weeks, we were assigned to a few cases for the practical session.
 |
| Case scenario |
 |
| 1st body |
 |
| The bodies are given according to the scenario |
 |
| we discussed and collected the evidence while writing the report |
 |
| behind the forensic building |
 |
| Our last CBD |
 |
| In front of the mortuary. The place is quite small, I wonder how they handled the bodies during Covid-19 era |
EMERGENCY POSTING (2 weeks) Example of cases triaged to Red Zone(taken from Medic USM website) :
- All chest pain.
- All referred cases of Acute Myocardial Infarction or Unstable Angina.
- All dyspnoea of saturation < 95% and respiration of 25 per min.
- All patients with Airway compromise. eg. gasping, severe maxillofacial injuries and comatosed patients.
- Severe Asthma and COAD
- All cardio respiratory patients.
- Shock e.g. hypovolemic or cardiogenic patients.
- BP of 220/130 without symptoms.
- High BP with symptoms and impending stroke or blurring of vision.
- Patients with BP Systolic 90 and below and Heart Rate of 120 and below.
- All cases of convulsions and fit.
- D/Stix High with CNS involvement.
- Abd. pain and unstable patient in shock.
- Triple A and suspected intra-abdo.injury.
- Fever with shock.
- All unstable Ectopic pregnancy.
- Bilateral fracture femur.
- Unstable pelvic fracture.
- Poly trauma patient.
- All trauma cases with chest injuries.
- All gunshot wound/penetrating wound in the neck, chest and abdomen.
- All head injuries with GCS of 13 and below.
- All cases of burns with Airway compromise e.g.facial and lower neck.
- All cases of third degree burns > 25% body surface and burns on face and throat.
- Victims of alleged drowning.
- All vascular injuries or impairment.
- Triple A (Abdominal Aortic Aneurysm) and intra abdominal injuries.
- Neonates and babies with HR of 210/min and RR 60/min or evidence of respiratory compromise, wheezing and stridor
Usually, we had lectures and seminar presentations in the morning or afternoon. We didn't have our own lecturer, so our university hired 2 specialists in HTAA to teach us. Both of them were so nice to us and helpful. We had practical sessions such as CPR, intubation, application of the cervical collar, logrolling, defibrillation, etc.
 |
| while waiting for practical session |
 |
| Our specialist explain the procedure |
 |
Practical for intubation
|
 |
| we practised intraosseous line insertion by using a chicken drumstick |
 |
| The specialist taught us by using this carpet : a practical session on the organization of medical care units in the disaster area such as collapsed building, motor vehicle accident which involve a high amount of casualties. |
 |
| cute right ! >_< |
 |
Triage and tagging of casualties :The classification or grouping of mass casualties based on the medical criterion of chance of survival (triage) is a necessary procedure when a large number of casualties must be cared for with limited medical resources, since most hospitals cannot accommodate stocks of supplies sufficient for dealing with public emergency conditions- credit to nzdl.org |
 |
| My hobby: capture as many as possible of sunset after coming back from the hospital |
 |
| The place that holds meaningful memories for 3 years |
 |
| post ED exam |
RADIOLOGY POSTING ( a.k.a. The eyes can't see what the mind doesn't know POSTING lol )
Radiology - Dr Aina, Dr Suzy, Dr Stephen, Dr Fara, Dr. Fatin, Dr. Zaza, etc
Radiology posting consists of a few branches: Mammography, X-ray, CT scan, MRI, Fluoroscopy, Ultrasound. We have to finish e rotation within 3 weeks.
We've been told by our seniors that we must be prepared mentally to enter this posting. I don't know why they said that. But, once I enter this posting, I truly understand why. The posting where every specialist is rushing to prepare a report for each imaging that were requested by each department in this hospital. Can you imagine how busy they are? Sometimes we witnessed a few HO's requests were rejected because the waiting line is soooo long for each department. Sometimes, their MO's need to go down to the radiology department to request by themselves for the sake of their patient. The Radio specialists did that because they have to prioritize which is the most important case that needs to do that imaging urgently.
We have to attach with the MO of each branch. You can't come to Radio empty-handed and empty-headed. At least carry some Radiology books with you (even though you don't know what you're reading haha but at least you have an effort tho) and PLEASE REVISE ANATOMY perfectly during this posting. The internet was quite slow because the location of the Radio dept seems like underground for me (haha) because I can't even see sunlight down there, so you better carry some anatomy notes along.
Xray dept was the most crowded one because patients were coming back and forth, so it's easier for us to fill up our Logbook. The view was so important, on how the radiographer took the X-ray. Either in AP/PA/lateral/OM. Also, the exposure, technique, light intensity, inhalation(CXR) are all important in every single film of xray
MRI was the least crowded place in this department. Because the patients came by appointment, only occasionally urgent cases were requested by the doctors in the ward. Because the imaging takes time about 1 hour for each case, We didn't get enough cases for our logbook throughout this posting, so the HOD insisted to extend our attachment just for us to finish the requirement in MRI. We learnt T1 weight, T2 weight, indications and contraindications in MRI.
In mammography, we were lucky because the doctors and the radiographer were so nice to us, so the doctors taught us several important points during the interpretation of mammograms. Only girls were allowed to observe how the mammography was done, so it was such an advantage for us. Honestly, the patient faced some discomfort while doing that procedure, but for the sake of breast cancer screening, they endured it.
Ultrasonography (USG) - one of the most difficult dept to enter cuz the MO's wouldn't allow us to attach with them unless we know the case and present it to them first. Otherwise, you will "kena halau" haha k please do not be afraid, it's just not my luck then. My friends just doing fine lol haha. Just pray a lot that you will meet with angelic MO, not the malignant one😅. Sometimes, I got the angelic MO's where they taught us a few things because clearly, we're noob students who just blankly stare at the black and white screen without knowing anything lol. We also got some opportunities to observe procedures such as abscess drainage from amoebic liver abscess with ultrasound guidance.
CT scan - the only thing I remembered about this department was a specialist scolded us because we attach with radiographer instead with MO's lol haha😂so please remember to get yourself attach with a doctor, not a radiographer. Furthermore, the doctor always asked us about the preparations of the patients before sending them to CT scan, such as why we need to stop Metformin and how it's related to the IV contrast given prior to the procedure.
The most important thing in Radio dept is you really need to know the INDICATIONS, CONTRAINDICATIONS, PREPARATION OF THE PATIENT before sending the patient for the procedure because it is the Houseman's job.
 |
| We were drilled by the specialist haha cuz we need to identify which part is abnormal in the HBS fluoroscopy. I don't know what the curse was cuz every time a student is called forward to identify the abnormal things on the film, we couldn't detect a single trace of abnormalities, but once we moved to the back, we noticed so many abnormalities. Conclusion: take a step back and look at the bigger picture. |
 |
| The moment of epiphany: The eyes can't see what the mind/brain doesn't know😅 |
 |
Our last lecture on Radio dept.
|
I was considering Radio as one of my options for my further studies [haha my friend gonna laugh at me kbye(but fr tho, Radio was quite interesting back then)]
CLINICAL LAB (1 Week )
This posting was just like a "Lawatan sambil belajar"😂 in Pathology dept and blood transfusion dept, but we learnt a lot in a week with lectures every day okay. I don't remember much during this posting, but I remembered all the specialists were super angelic😇
 |
| Blood Culture and sensitivity in the medium agar |
 |
| I don't remember exactly this thing but there is blood in each tube (anyone who know, please comment below) |
 |
| All gram stains and each bacteria |
PALLIATIVE POSTING (2 Weeks)
This is one of the calmest & most silent ward I ever came. The staffs here were all calm and helpful including our favourite specialist, Dr Katrina. Dulu pernah terfikir nak jadi macam Dr. Katrina, tp, sebab kena lalu Medical dulu utk masuk Palliative, so sis batalkan dulu niat tu😭
We became extremely cautious of whatever sounds we make once we enter this ward because this ward is the place where all the end-stage cancer patients were located. So, most of them were receiving supportive treatment like medication to relieve pain, fluids, etc. Almost every day we observed at least one of the patients pass away. Such a heartbreaking moment😢
 |
| Dr. Katrina taught us the progression of cancer with a CT scan of one of our patients |
 |
| while waiting for lecture & BST |
ENT POSTING (3 WeekS )
ENT : Ear, Nose & Throat (Otorhinolaryngology)
This was one of the best postings I ever had because the specialists were all sporting !
Mostly we attached with the specialist in the clinic or we enter Operation Théâtre once a week. During afternoon, we got lectures/seminar in the seminar room in ENT department.
 |
| Otorhinolaryngoscope - each specialist's room got this equipment so we observed as many as possible cases each day |
Some of the cases were seen by me. Actually, they were a lot, but I can't remember much thou😅
-Hallpike manoeuvre
I still remember the Rhinolith smell and how it was crushed by our specialist under local anaesthesia in the clinic. The patient complained that her whole house has a foul smell like a corpse, but then the culprit was something inside her nasal cavity.
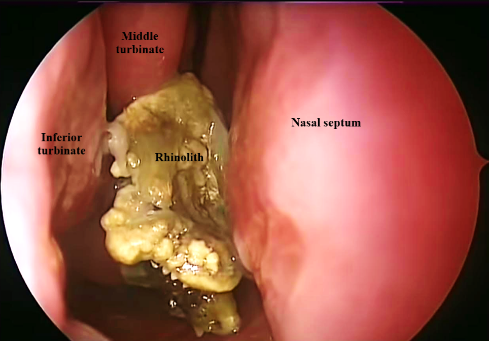 |
| rhinolith |
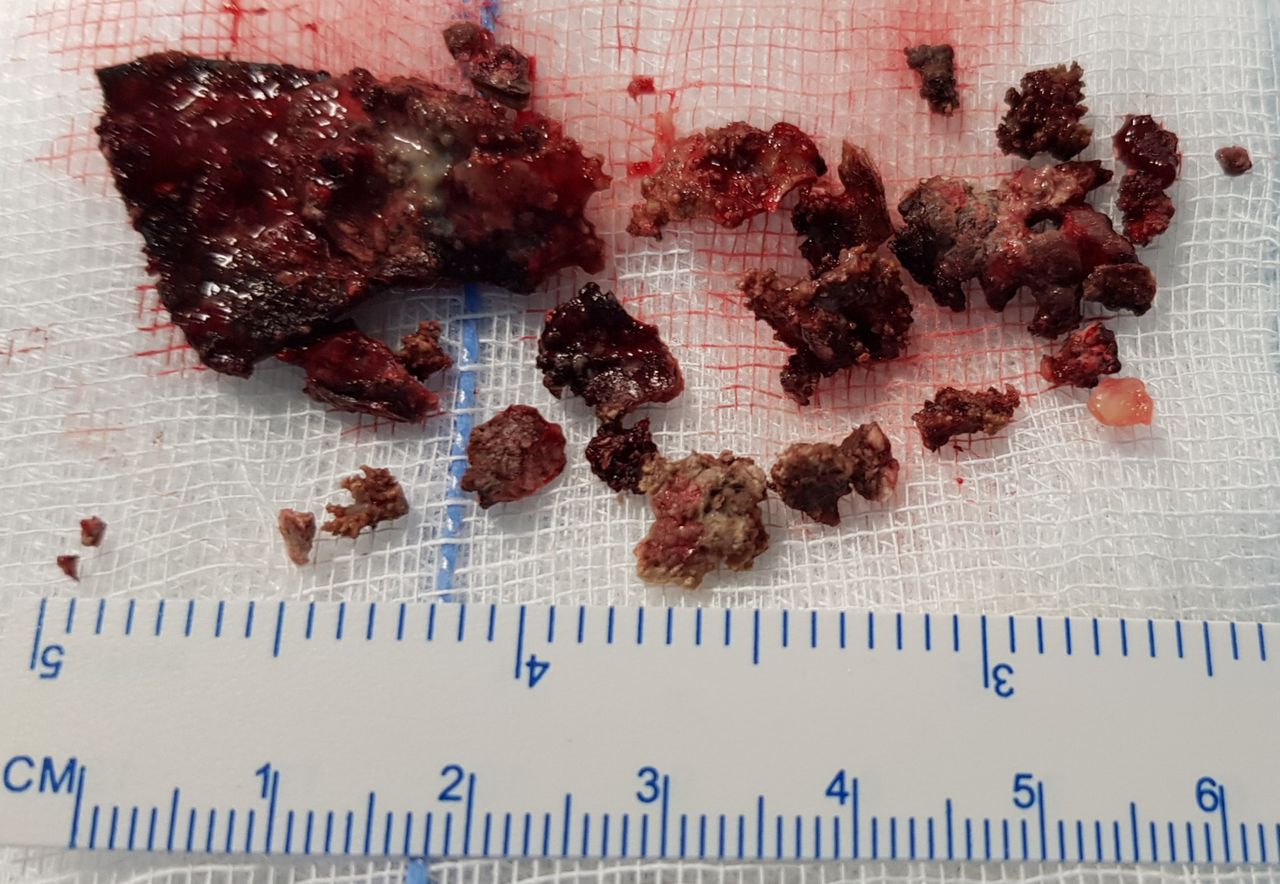 |
| rhinolith |
FEES(Flexible/fiberoptic endoscopy evaluation of swallowing) was done every time before the nasogastric tube is taken off, usually in stroke patients in which cranial nerves involved with swallowing were affected. You can read the details about FEES here : WHAT IS FEES?  |
| Usually, the patient is asked to swallow a coloured liquid to ensure the liquid is seen clearly, if the patient passed this test by not choking, then NG tube can be stopped |
 |
This is one of the procedures we observed in ENT : a pseudocyst. after aspiration of cyst, the cyst is made to remain collapsed by applying buttons on both sides fixed by trans pinna suturing(read more here)
Don't be mistaken, this is one of the most efficient way for the treatment so that the cyst filled with fluid didn't recur again |
I took an opportunity as a medical student to do a free check-up for my allergic rhinitis. A rhinoscope was inserted into my nasal cavities and the feel was ughhh haha it was not that bad as swab for Covid-19 but still, I sneezed just after the scope is taken out 😂fortunately, I got a nasal spray and antihistamine for my AR. Here, a sneak peek inside a nasal cavity :
 |
| My first nasal spray. Thank you Dr. Khairul ! (Dr. yg plg bapak2 sgt kat ENT) |
 |
| Photo session with all the sporting specialists (Dr. Najeb ajak buat "ORANGE" x ingat apa variety show yg anak dia tengok haha😂😂) |
 |
| Our last lecture with Paediatrics ENT Specialist Dr Suhaimi(a.k.a. Doraemon enthusiast😂)😭😭😭😭😭sedih sebab ENT is one of my happiest moments waktu year 4 dulu2 |
OPHTHALMOLOGY POSTING (3 Weeks )
Ophthal- Dr Rohana, Dr Wan, Dr Akmal, Dr Rini, Dr Fatimah, Dr. Sarah, Dr.Wardati, Dr Rudi, etc.
In this posting, most of the time we attached with the specialists/MO in clinic. Sometimes, we went to OT and ward on rotation.
In ophthal ward is kinda different from the other ward not only because this is the most "lengang" & peaceful ward, but the ward round was held in the procedure room. Usually, the specialist will come to the patient's bed, but it happened the other way around in ophthal ward which is the patients will come into the procedure room because the specialist will only check their eyes by using a slit lamp. The specialists were kind and usually will let us observe the abnormalities of the patient's eyes during ward round so please don't miss the ward round on 7.30am every morning(if I'm not mistaken).
In OT, usually, we only observed OT on the screen because the camera on the surgeon's head is projected into a screen.
Usually, we need at least 1 ophthalmoscope for each group because the teaching involved ophthalmoscope most of the time. So we bought one for our group because, during our time, our university didn't provide it (p.s : WiMed please do sth about it ok !😂We already did sth, but yeah....)
 |
| I & Han used our PTPTN money to buy this otoscope & ophthalmoscope set😂 |
If anyone is interested to rent my ophthalmoscope please read this entry : rent ophthalmoscope here(KL & Selangor only, no postage)
Sometimes, we became a mock exam patient for Master students :
 |
| Practice for a master student especially those who wear spectacles, some of our cases are bizarre, so it's good for their practice |
 |
| Our last lecture with Dr. Rini. p.s. : muka sis penat sebab jadi leader masa ni, pening uruskan anak2 haha |
Most of the specialists here is female doctors, only a few of them are male doctors. So the specialists here all were soft-spoken and gentle towards patients. I was considering ophthal as one of my choices in the future because my mother insisted me to become one of them😂, but I don't know yet what will happen in the future so I'll just leave it to Allah to decide😇.








































































































Comments
Post a Comment